In my own personal growth as a pro-life advocate, my arguments were not always so solid or well thought out. Instead, they were full of emotion, such as anger, hate and impulsive accusations. I have also never done very well in confrontational situations, which I'm sure many of you can relate to, so I would often back down if the argument ever got too heated.

As I grew, I came to realize that no one was having any sort of moral epiphany based on my emotionally driven rants. So, I began to contemplate on how I could put my emotions into meaningful words. I started to learn everything I could about the pro-life movement; finding evidence to support my arguments and using my own medical experience to justify my stance against abortion. I, also, observed how other pro-lifers interacted with pro-choice commentators and saw which approaches worked better than others. Religous based comments, for example, such as "God sees all" or "you will be judged at the end of days" had either a provoking effect or no affect at all on the opposing side; particularly with those from the younger generations (ie. Millennials). Even many pro-life Millennials (such as myself) avoided bringing religion into the debate and, instead, resorting to a more deductive approach; such as a the question/answer format. For example: "If abortion is a choice, then why doesn't the father or child get to choose? This allows the other side to truly think about their argument and come up with their own evidence, if any, to support it.
Below, I have constructed some of the more familiar and commonly used arguments used by pro-choice/pro-abortion advocates and provided evidence exposing their fallacies:
1. "YOU CAN'T TELL ME WHAT TO DO WITH MY BODY!" "MY BODY, MY CHOICE!"

Any variation of this argument I'm sure you've seen or heard. I'm usually thinking "that's great, if it was "your body" we were actually talking about."
If we look at human anatomy, what separates the baby from the mother is the placenta. The placenta attaches to the endometrial lining of the uterus and forms this capillary-like network (almost like a root system) between the blood vessels of placenta and the blood vessels in the mother's uterus. This allows the mother's blood to be filtered of everything the baby needs to grow and mature (ie. nutrients and oxygen), while keeping out the harmful stuff, like the majority of the mother's immune cells (all expect the IgG antibody), which would see the baby as "foreign" and attack. The baby is, therefore, only physically attached to the placenta and not the mother. If the baby was actually part of the mother's body, then the child would be able to grow and develop anywhere within the her body and Not be seen as a foreign entity by her immune system.

In this picture, we see the blood vessel (or vascular) network between the placenta and the mother's vessels.



Here, is a depiction of the mother's immune cells being filtered out, so that they will not attack the baby; which is seen as foreign.

This is what an actual, single-disc placenta looks like. They house and protect the unborn child, until they are ready to thrive outside the womb. Once the baby is born, the placenta detaches from the uterus and the uterus contracts and shrinks to its original position and size.
Short Answer: The baby's body is not part of the mother's body. The child is only physically attached to the placenta, which separates the baby from the mother and her immune system, which sees the baby as a foreign. The uterus is, also, not a vital organ necessary for the mother's survival. It's sole purpose is to sustain and protect the growth and development of a human child. Therefore, the uterus exists solely for the child, not the mother. If anyone holds claim to it, then it would be the baby.
2. ABORTION SHOULD BE LEGAL IN CASES OF RAPE OR INCEST!
Rape (comprising 1%-3% of abortion cases) is an undeniably horrific and barbaric violation of the human body. The punishments administered for such crimes are grievously insufficient to the mental, spiritual and physical damage that is done to one person. Sometimes, however, a third victim is created; a child. This child, has no involvement in the circumstances that surround their conception; nor do they have any control over them. Yet, they are treated and punished at the same level as their mother's rapist. To some, "getting rid of" this child through abortion supposedly heals the mother from her rape. Abortion, however, does not have the power to erase rape. Instead, it merely compounds the crime by adding the death of an innocent child. The mother, then, not only has her rape to carry with her but, also, the death of her child.

Children conceived in rape or incest are not their mother's rapist, nor will they ever grow up to be a rapist. They are fully functioning human beings, capable of amounting to anything they desire.
Instead of pushing the idea that abortion will help heal from a rape, we need to pull from every therapeutic support system available for these mothers and their babies. We need to let her know that her child is also a victim and separate her child from her rapist. As hundreds of mothers have attested to after choosing life for their children conceived in rape; giving life was, in itself, a way for them to heal together. Please read their stories below:
Read some of their stories here:
-I Am Raising the Daughter of A Man Who Raped Me
-‘It was a mass production line:’ Women tell stories of bad abortion facilities
-I was conceived in rape, but my life has dignity and value
-I was raped while homeless, but my daughter is a gift
-Raped by relatives, Wendi refused abortion and is raising her daughter on her own
-Raped as a teen, I chose life for my daughter and never looked back
-Pregnant at 12 after a brutal rape, she rejected abortion. Now, she has no regrets.
-Can You Love a Child of Rape?
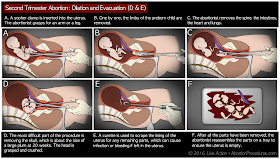
3. OUTLAWING ABORTION WOULD DRIVE WOMEN TO UNSAFE, BACK-ALLY ABORTIONS OR TO USING HANGERS; CAUSING MORE WOMEN TO DIE!
Most women who feel that they NEED to have an abortion believe it to be their ONLY option. Some of the most common reasons women give for wanting an abortion are: financial stresses, pressure from a significant other, family and/or friends, instability within the home (ie abuse, marital problems), a break-down in their support system (ie. friends and family), education (currently in school), age (too young or too old), just had a baby or already have too many kids, mom has a medical or mental problem, the baby was diagnosed with a disability, single mom, or they had an undisclosed affair.

Social factors also seem to play a significant role in a mother's decision. For example, some women claim that they don't want to be pregnant because they would look fat in a bathing suit. Others, however, have less superficial reasonings, such as: the social pressures against teen pregnancy and older mothers, or pregnancy out of wed-lock. There's even those judgmental remarks against mothers with multiple children (I got one from an older woman who said "enough is enough"-sheesh!). Whatever the reason, there is help and support for women from all backgrounds. Life affirming/crisis pregnancy centers, for instance, aim to eliminate the causative agent that drives a woman to want abortion. They strive to provide the resources and support the mother and her family needs in order to choose life for her child and and they lay out every option available to her. Because, how can you make a "choice" if you aren't given every option out there? Also, against popular belief, these centers extend their help beyond the pregnancy; helping mothers and families long after birth. Most of these centers also offer post-abortive counseling to those struggling with any past abortions.

For those who firmly believe that prohibiting access to abortion will lead to higher maternal mortality rates (aka maternal death rates), a 50 year study in Chile, between 1957–2007, published on May 4, 2012, identified factors related to maternal mortality reduction within their country. During their study, the maternal mortality rate in Chile had decreased from 293.7 to 18.2/100,000 live births, a decrease of 93.8%. Even after abortion was prohibited in 1989, the mortality rate still continued to decrease from 41.3 to 12.7 per 100,000 live births (−69.2%). The authors concluded that increasing education level drastically impacted the downward trend in the maternal mortality rate, along with other key factors, such as access and utilization of maternal health facilities, changes in women's reproductive behavior and improvements of the sanitary system.
 "Pie chart A represents the period from 1958 to 1962; B period from 1971 to 1075; C period from 1985 to 1989; and D period from 2003 to 2007. Each period shows the five major causes of maternal mortality according to international codes of disease." (Elard Koch et al., May 4, 2012).
"Pie chart A represents the period from 1958 to 1962; B period from 1971 to 1075; C period from 1985 to 1989; and D period from 2003 to 2007. Each period shows the five major causes of maternal mortality according to international codes of disease." (Elard Koch et al., May 4, 2012).
Therefore, making abortion illegal would not cause an increase in maternal death rate if the necessary resources and supplies were easily accessible to the public. This is why having funds transferred away from abortion giants, like Planned Parenthood, to Federally Qualified Health Centers is so important. Women need proper resources and support, not abortion to solve their problems! Additionally, we need to focus on higher education output and promote the proper use of contraceptives and safer sex practices. Because, the more you know, the better decisions you make.
Furthermore, the United States is one of the only industrialized countries without guaranteed paid maternity leave. Most US companies do provide anywhere from 6-12 weeks off, however; but, pay is usually supplemented by sick/vacation time and short term disability, after being employed for a certain amount of time. Most households, like ours, are unable to live off of one income alone, forcing mothers to return to work prematurely. I, for one, only had 2 weeks off with my first child and 6 weeks with my second and I threw up four times my first day back to work after giving birth to my second. Situations like these are what's failing mothers and their children. We need to demand that our government officials provide our citizens with the tools and resources they need to raise a family. Our country is lacking in this aspect and it desperately needs to change.
Short Answer: More women will not die if abortions were ever made illegal; just as long as the resources, education and support they need are easily accessible and available. Funding to the proper crisis health centers and increased paid maternity leave will help alleviate that. Legality also does not guarantee safety. Many women have died from legally performed abortions every year, as we've seen from "The House of Horrors" with Kermit Gosnell and from the many women listed on Operation Rescue.
4. "ABORTIONS ARE SAFER THAN GIVING BIRTH!"
Every year, the CDC collects and reports abortion statistics from 52 areas (50 US states plus the District of Columbia and New York City). From those 52 areas, ONLY 47 have submitted their data from the years 2004-2013. Those not included are: California, Louisiana, Maryland, New Hampshire, and West Virginia. Why? Because, all data from each state are voluntarily submitted! With California being one of the largest abortion providers, next to New York, you can see how obviously inaccurate any conclusions made from this data would be.

Data on live-births, on the other hand, are more numerous, with the number of live births greatly outnumbering the number of documented abortions. When the CDC calculates the number of deaths due to pregnancy complications, they request the 52 reporting areas to voluntarily send copies of death certificates for all women who have died during pregnancy or within 1 year of pregnancy, along with copies of matching birth or fetal death certificates. All of the information is then collected and summarized, with a medically trained epidemiologists there to determine the cause and time of death related to the pregnancy. Causes of deaths are, then, coded through a system established in 1986 by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention Maternal Mortality Study Group. The number of pregnancy-related deaths are then compared to 100,000 live births to form their ratio.
Included on the list of cause of deaths from 2011-2013, for instance, are:
Cardiovascular diseases, 15.5%.
Non-cardiovascular diseases, 14.5%.
Infection or sepsis, 12.7%.
Hemorrhage, 11.4%.
Cardiomyopathy, 11.0%.
Thrombotic pulmonary embolism, 9.2%.
Hypertensive disorders of pregnancy, 7.4%.
Cerebrovascular accidents, 6.6%.
Amniotic fluid embolism, 5.5%.
Anesthesia complications, 0.1%.
Unknown cause of death, 6.2%.
The CDC defines a pregnancy-related death as "the death of a woman while pregnant or within 1 year of pregnancy termination–regardless of the duration or site of the pregnancy–from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes." Based on this statement, things like ectopic pregnancies and miscarriages are included in these percentages, thus giving an inaccurate portrayal of birth-related maternal death rates. Additionally, contributing factors, like pre-existing conditions or outside influences, such as influenza outbreaks and, currently, zika, further skew these numbers.
As we all know, abortions carry numerous complications, such as: inflammation/infection/sepsis, hemorrhaging/blood loss, punctured uterus, incomplete abortions leading to the first symptoms listed, scarring leading to infertility, subsequent ectopic pregnancies, miscarriages and/or premature births, increased rates of breast cancer, and psychological effects-suicide/depression. If not documented properly by hospital staff or its affiliates, these complications would further skew any ratios related to abortion and/or live births. Not to mention the fact that patients may not always be truthful with regards to their reproductive history.


In summary, the number of maternal deaths related to pregnancy/birth are based on incomplete, voluntarily provided data with way too many variables, such as the possible inclusion of secondary abortion-related complications (which can manifest years later) and the definite inclusion of ectopic pregnancies and miscarriages. We also see 6.1% of cases listed under unknown cause of death. Therefore, we can clearly deduce that death from giving birth is not accurately portrayed here.
Additionally, abortion has never been a safe procedure. WHO claims that 13% of worldwide abortions result in maternal death. However, they attribute this rate to the abortion being performed "unsafely." As I've stated before, there are many risk factors and secondary symptoms that come with every abortion; not to mention the guaranteed death of another human being. There is nothing safe about that! Nevertheless, the abortion industry likes to use these percentages to keep abortion legal, accessible and funded internationally. Any laws made to restrict abortion in any way are quickly struck down; including those that would actually improve patient safety in the US.

Because of their high influences within political parties and many affiliates, the abortion industry remains profoundly unregulated; with most abortion facilities not even required to follow the same basic safety standards as any out-patient facility. When a recent US Texas bill was put forth to increase patient safety protocols, the abortion industry, once again, claimed that the law would place an "undue burden" on women's access to abortion. Since there are very little laws governing these abortion facilities, that means no real health inspections, no real patient safety standards and no obligation to provide these mother's with all of the information regarding the gestational development of their unborn child nor any complications that will arise from the abortion procedure. Many of these women are kept in the dark when it comes to abortion and it is all completely done legally.
Below are two articles describing some of the horrendous conditions found during police inspections at legally operating abortion facilities:
Abortion Industry Negligence Nationwide: Highlighting the Most Egregious Offenses, Nurses describe ‘unsafe’ conditions at Delaware abortion clinic
5. "A FETUS IS NOT A REAL PERSON; JUST A BLOB OF CELLS"
I've personally had a young girl call an unborn child "just medical waste," during one of my many debates on social media. To call an unborn child a "blob of cells" is so profoundly ignorant and uneducated, yet we hear it, and statements like it, consistently recited all over social media and TV series, like: Super Store, The Magicians, Jessica Jones, Blind spot, Scandal, Orange is the New Black, Jane the Virgin, You're The Worst, Crazy Ex-Girlfriend etc.
The belief that an unborn child is Not a Person, worthy of rights and protection, is the Heart of the Pro-choice/Pro-abortion stance. Most often, these beliefs have absolutely nothing to do with Choice; especially since True Choice would technically involve the opinion of the father and that of the child. But, by believing that these children are Not Human, it takes away any emotional or moralistic involvement with ending another person's life. We could toss blame at the profound lack of high school education within the areas of human reproduction and development, or we could say that the over-promotion of abortion as a "safe and legal procedure," merely removing a chunk of tissue is at fault. Or, maybe it's both!
To alleviate some of this education deficiency, I am providing a brief, general overview on Reproductive Anatomy & Development. To start, lets take a look at the Human Uterus.

2. ABORTION SHOULD BE LEGAL IN CASES OF RAPE OR INCEST!
Rape (comprising 1%-3% of abortion cases) is an undeniably horrific and barbaric violation of the human body. The punishments administered for such crimes are grievously insufficient to the mental, spiritual and physical damage that is done to one person. Sometimes, however, a third victim is created; a child. This child, has no involvement in the circumstances that surround their conception; nor do they have any control over them. Yet, they are treated and punished at the same level as their mother's rapist. To some, "getting rid of" this child through abortion supposedly heals the mother from her rape. Abortion, however, does not have the power to erase rape. Instead, it merely compounds the crime by adding the death of an innocent child. The mother, then, not only has her rape to carry with her but, also, the death of her child.

Children conceived in rape or incest are not their mother's rapist, nor will they ever grow up to be a rapist. They are fully functioning human beings, capable of amounting to anything they desire.
Instead of pushing the idea that abortion will help heal from a rape, we need to pull from every therapeutic support system available for these mothers and their babies. We need to let her know that her child is also a victim and separate her child from her rapist. As hundreds of mothers have attested to after choosing life for their children conceived in rape; giving life was, in itself, a way for them to heal together. Please read their stories below:
Read some of their stories here:
-I Am Raising the Daughter of A Man Who Raped Me
-‘It was a mass production line:’ Women tell stories of bad abortion facilities
-I was conceived in rape, but my life has dignity and value
-I was raped while homeless, but my daughter is a gift
-Raped by relatives, Wendi refused abortion and is raising her daughter on her own
-Raped as a teen, I chose life for my daughter and never looked back
-Pregnant at 12 after a brutal rape, she rejected abortion. Now, she has no regrets.
-Can You Love a Child of Rape?
3. OUTLAWING ABORTION WOULD DRIVE WOMEN TO UNSAFE, BACK-ALLY ABORTIONS OR TO USING HANGERS; CAUSING MORE WOMEN TO DIE!
Most women who feel that they NEED to have an abortion believe it to be their ONLY option. Some of the most common reasons women give for wanting an abortion are: financial stresses, pressure from a significant other, family and/or friends, instability within the home (ie abuse, marital problems), a break-down in their support system (ie. friends and family), education (currently in school), age (too young or too old), just had a baby or already have too many kids, mom has a medical or mental problem, the baby was diagnosed with a disability, single mom, or they had an undisclosed affair.

Social factors also seem to play a significant role in a mother's decision. For example, some women claim that they don't want to be pregnant because they would look fat in a bathing suit. Others, however, have less superficial reasonings, such as: the social pressures against teen pregnancy and older mothers, or pregnancy out of wed-lock. There's even those judgmental remarks against mothers with multiple children (I got one from an older woman who said "enough is enough"-sheesh!). Whatever the reason, there is help and support for women from all backgrounds. Life affirming/crisis pregnancy centers, for instance, aim to eliminate the causative agent that drives a woman to want abortion. They strive to provide the resources and support the mother and her family needs in order to choose life for her child and and they lay out every option available to her. Because, how can you make a "choice" if you aren't given every option out there? Also, against popular belief, these centers extend their help beyond the pregnancy; helping mothers and families long after birth. Most of these centers also offer post-abortive counseling to those struggling with any past abortions.

For those who firmly believe that prohibiting access to abortion will lead to higher maternal mortality rates (aka maternal death rates), a 50 year study in Chile, between 1957–2007, published on May 4, 2012, identified factors related to maternal mortality reduction within their country. During their study, the maternal mortality rate in Chile had decreased from 293.7 to 18.2/100,000 live births, a decrease of 93.8%. Even after abortion was prohibited in 1989, the mortality rate still continued to decrease from 41.3 to 12.7 per 100,000 live births (−69.2%). The authors concluded that increasing education level drastically impacted the downward trend in the maternal mortality rate, along with other key factors, such as access and utilization of maternal health facilities, changes in women's reproductive behavior and improvements of the sanitary system.

Therefore, making abortion illegal would not cause an increase in maternal death rate if the necessary resources and supplies were easily accessible to the public. This is why having funds transferred away from abortion giants, like Planned Parenthood, to Federally Qualified Health Centers is so important. Women need proper resources and support, not abortion to solve their problems! Additionally, we need to focus on higher education output and promote the proper use of contraceptives and safer sex practices. Because, the more you know, the better decisions you make.
Furthermore, the United States is one of the only industrialized countries without guaranteed paid maternity leave. Most US companies do provide anywhere from 6-12 weeks off, however; but, pay is usually supplemented by sick/vacation time and short term disability, after being employed for a certain amount of time. Most households, like ours, are unable to live off of one income alone, forcing mothers to return to work prematurely. I, for one, only had 2 weeks off with my first child and 6 weeks with my second and I threw up four times my first day back to work after giving birth to my second. Situations like these are what's failing mothers and their children. We need to demand that our government officials provide our citizens with the tools and resources they need to raise a family. Our country is lacking in this aspect and it desperately needs to change.
Short Answer: More women will not die if abortions were ever made illegal; just as long as the resources, education and support they need are easily accessible and available. Funding to the proper crisis health centers and increased paid maternity leave will help alleviate that. Legality also does not guarantee safety. Many women have died from legally performed abortions every year, as we've seen from "The House of Horrors" with Kermit Gosnell and from the many women listed on Operation Rescue.
4. "ABORTIONS ARE SAFER THAN GIVING BIRTH!"
Every year, the CDC collects and reports abortion statistics from 52 areas (50 US states plus the District of Columbia and New York City). From those 52 areas, ONLY 47 have submitted their data from the years 2004-2013. Those not included are: California, Louisiana, Maryland, New Hampshire, and West Virginia. Why? Because, all data from each state are voluntarily submitted! With California being one of the largest abortion providers, next to New York, you can see how obviously inaccurate any conclusions made from this data would be.
Data on live-births, on the other hand, are more numerous, with the number of live births greatly outnumbering the number of documented abortions. When the CDC calculates the number of deaths due to pregnancy complications, they request the 52 reporting areas to voluntarily send copies of death certificates for all women who have died during pregnancy or within 1 year of pregnancy, along with copies of matching birth or fetal death certificates. All of the information is then collected and summarized, with a medically trained epidemiologists there to determine the cause and time of death related to the pregnancy. Causes of deaths are, then, coded through a system established in 1986 by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention Maternal Mortality Study Group. The number of pregnancy-related deaths are then compared to 100,000 live births to form their ratio.
Included on the list of cause of deaths from 2011-2013, for instance, are:
Cardiovascular diseases, 15.5%.
Non-cardiovascular diseases, 14.5%.
Infection or sepsis, 12.7%.
Hemorrhage, 11.4%.
Cardiomyopathy, 11.0%.
Thrombotic pulmonary embolism, 9.2%.
Hypertensive disorders of pregnancy, 7.4%.
Cerebrovascular accidents, 6.6%.
Amniotic fluid embolism, 5.5%.
Anesthesia complications, 0.1%.
Unknown cause of death, 6.2%.

The CDC defines a pregnancy-related death as "the death of a woman while pregnant or within 1 year of pregnancy termination–regardless of the duration or site of the pregnancy–from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes." Based on this statement, things like ectopic pregnancies and miscarriages are included in these percentages, thus giving an inaccurate portrayal of birth-related maternal death rates. Additionally, contributing factors, like pre-existing conditions or outside influences, such as influenza outbreaks and, currently, zika, further skew these numbers.
As we all know, abortions carry numerous complications, such as: inflammation/infection/sepsis, hemorrhaging/blood loss, punctured uterus, incomplete abortions leading to the first symptoms listed, scarring leading to infertility, subsequent ectopic pregnancies, miscarriages and/or premature births, increased rates of breast cancer, and psychological effects-suicide/depression. If not documented properly by hospital staff or its affiliates, these complications would further skew any ratios related to abortion and/or live births. Not to mention the fact that patients may not always be truthful with regards to their reproductive history.


In summary, the number of maternal deaths related to pregnancy/birth are based on incomplete, voluntarily provided data with way too many variables, such as the possible inclusion of secondary abortion-related complications (which can manifest years later) and the definite inclusion of ectopic pregnancies and miscarriages. We also see 6.1% of cases listed under unknown cause of death. Therefore, we can clearly deduce that death from giving birth is not accurately portrayed here.
Additionally, abortion has never been a safe procedure. WHO claims that 13% of worldwide abortions result in maternal death. However, they attribute this rate to the abortion being performed "unsafely." As I've stated before, there are many risk factors and secondary symptoms that come with every abortion; not to mention the guaranteed death of another human being. There is nothing safe about that! Nevertheless, the abortion industry likes to use these percentages to keep abortion legal, accessible and funded internationally. Any laws made to restrict abortion in any way are quickly struck down; including those that would actually improve patient safety in the US.


Because of their high influences within political parties and many affiliates, the abortion industry remains profoundly unregulated; with most abortion facilities not even required to follow the same basic safety standards as any out-patient facility. When a recent US Texas bill was put forth to increase patient safety protocols, the abortion industry, once again, claimed that the law would place an "undue burden" on women's access to abortion. Since there are very little laws governing these abortion facilities, that means no real health inspections, no real patient safety standards and no obligation to provide these mother's with all of the information regarding the gestational development of their unborn child nor any complications that will arise from the abortion procedure. Many of these women are kept in the dark when it comes to abortion and it is all completely done legally.
Below are two articles describing some of the horrendous conditions found during police inspections at legally operating abortion facilities:
Abortion Industry Negligence Nationwide: Highlighting the Most Egregious Offenses, Nurses describe ‘unsafe’ conditions at Delaware abortion clinic
5. "A FETUS IS NOT A REAL PERSON; JUST A BLOB OF CELLS"
I've personally had a young girl call an unborn child "just medical waste," during one of my many debates on social media. To call an unborn child a "blob of cells" is so profoundly ignorant and uneducated, yet we hear it, and statements like it, consistently recited all over social media and TV series, like: Super Store, The Magicians, Jessica Jones, Blind spot, Scandal, Orange is the New Black, Jane the Virgin, You're The Worst, Crazy Ex-Girlfriend etc.
The belief that an unborn child is Not a Person, worthy of rights and protection, is the Heart of the Pro-choice/Pro-abortion stance. Most often, these beliefs have absolutely nothing to do with Choice; especially since True Choice would technically involve the opinion of the father and that of the child. But, by believing that these children are Not Human, it takes away any emotional or moralistic involvement with ending another person's life. We could toss blame at the profound lack of high school education within the areas of human reproduction and development, or we could say that the over-promotion of abortion as a "safe and legal procedure," merely removing a chunk of tissue is at fault. Or, maybe it's both!
To alleviate some of this education deficiency, I am providing a brief, general overview on Reproductive Anatomy & Development. To start, lets take a look at the Human Uterus.

The Uterus is a reproductive organ that resides within the pelvic cavity of the female body. It sits between the rectum and the urinary bladder, with the main portion of the uterus actually "cupping," or laying on top of the urinary bladder. This is why, during pregnancy, a baby's kick can send a mother flying to the bathroom, or why a mother may have the sensation to poop during labor.


Looking at an upright, cut view of the uterus, we see a nicely labeled diagram distinguishing the many different parts of the organ. We see the 3 named areas of the Fallopian Tube (where fertilization and cell division first takes place), the different parts of the uterus itself: the Endometrium (a blood-vessel rich area that is shed and exposed during our periods and is the site for implantation during pregnancy), the Myometrium (the thick muscular portion of the uterus that contracts during menstruation and labor, giving us that wonderful cramping feeling) and the outer serosal covering, or parametrium, of the uterus itself. The cervix, attached to the lower portion of the uterus, partially resides within the vagina and is surrounded by vaginal mucosa. During labor, the cervix naturally dilates and thins (or efaces) to allow your baby to pass through. During an abortion, the doctor artificially dilates the cervix enough to fit their tools into the uterus to either suction or dismember your child.
Now, lets review Human Gestation
A human being literally develops from a single cell into a multi-cellular organism in ONLY 9 months! This process is performed at an immensely fast rate and with such efficiency that it's a wonder why we don't see more go wrong. Yes, specific abnormalities do occur, but, considering everything that must be completed in such a short amount of time, you would expect more abnormalities to occur more often. It's actually nothing short of astonishing!
Here are some terms to become familiar with:
- Week 1-8 is known as the Embryonic Period (The most important period)
- Week 9 up to Birth is known as the Fetal Period
- The first Month after birth is known as the Neonatal Period

During the Embryonic Period (week 1-8, or 56 days) your baby is called an Embryo. During this time, 90% of their organ systems and structures become established. Cells divide, move around and mature to become specific cells (ie. skin cells, heart cells, bone cells etc.) and all of this occurs at an extremely fast rate. These first 8 weeks are considered the most vulnerable portions of the pregnancy, since most abnormalities that can possibly occur, do so during this time.
During the Fetal Period (week 9 up until birth) your baby is called a Fetus (Latin for bring forth your young). During this time, the organs that were formed during the embryonic period grow and mature.
Now, lets take a look at what happens week-by-week:
Week 1: The first week of the embryonic period begins with fertilization. The embryo, then, becomes a Zygote, then a Morula, and finally a Blastocyst. Since so much occurs within this first week, the details of this process are split up into days. See below:

Day 1 (Fertilization): Fertilization takes just over 24 hours to complete and normally takes place in the part of the Fallopian Tube closest to the ovary. Fertilization occurs when sperm and egg fuse to form a new, genetically distinct male or female organism. In this first stage, the embryo, complete with two sets of DNA, is formally called a Zygote.


Day 2-3: The Zygote then enters into continuous cell division as it travels down the Fallopian Tube towards the uterus. When it reaches to about 12-32 cells, it is now formally called a Morula and measures only 0.1 to 0.2 mm. These individual cells (also known as Blastomeres) are in a compact ball, which are held together by a protective membrane called the zona pellucida (ie. like a balloon holding together a bunch of marbles).


Day 4: Fluid, then, begins to fill inside the ball of cells, creating a fluid-filled space called a blastocystic cavity. Because of the fluid, the dividing cells are pushed aside and form into two different groups: the first (outer) group will be responsible for implanting into the uterus and forming the placenta, while the second (inner) group of cells are responsible for forming your baby. The Embryo is now formally called a Blastocyst and has entered the inside of the Endometrium of the Uterus.


Day 5-6: The zona pellucida (the outer covering) then breaks open and the cells (now numbering over 100) move out, or "hatch" and get ready to implant into the uterus.
 Numbers 2, 3 & 5 are the dividing cells, Number 4 is the fluid filled space, and Number 1 is the Zona Pellucida.
Numbers 2, 3 & 5 are the dividing cells, Number 4 is the fluid filled space, and Number 1 is the Zona Pellucida.
Day 7 (Implantation): The embryo implants into the endometrial lining of the uterus and burrows until it is protectively covered by the endometrium. This process continues into the second week of pregnancy.


Number 9 is the endometrial plug completely covering the implanted embryo and keeping it protected and Number 8 & 11 are the inner and outer layers of cells.

The cells that form your baby continue to divide and organize into two distinct layers. The outer layer of cells, called the epiblast (the blue cells in the picture) and the inner layer of cells called the hypoblast (the yellow cells in the picture). At the end of this week, a long streak appears in the middle of the epiblast layer (much like a long gap), called the primitive streak. The cells from the epiblast layer move into this streak to form a third, middle layer of cells (see the 4th picture below).


A human being literally develops from a single cell into a multi-cellular organism in ONLY 9 months! This process is performed at an immensely fast rate and with such efficiency that it's a wonder why we don't see more go wrong. Yes, specific abnormalities do occur, but, considering everything that must be completed in such a short amount of time, you would expect more abnormalities to occur more often. It's actually nothing short of astonishing!
Here are some terms to become familiar with:
- Week 1-8 is known as the Embryonic Period (The most important period)
- Week 9 up to Birth is known as the Fetal Period
- The first Month after birth is known as the Neonatal Period

During the Embryonic Period (week 1-8, or 56 days) your baby is called an Embryo. During this time, 90% of their organ systems and structures become established. Cells divide, move around and mature to become specific cells (ie. skin cells, heart cells, bone cells etc.) and all of this occurs at an extremely fast rate. These first 8 weeks are considered the most vulnerable portions of the pregnancy, since most abnormalities that can possibly occur, do so during this time.
During the Fetal Period (week 9 up until birth) your baby is called a Fetus (Latin for bring forth your young). During this time, the organs that were formed during the embryonic period grow and mature.
Now, lets take a look at what happens week-by-week:
Week 1: The first week of the embryonic period begins with fertilization. The embryo, then, becomes a Zygote, then a Morula, and finally a Blastocyst. Since so much occurs within this first week, the details of this process are split up into days. See below:

Day 1 (Fertilization): Fertilization takes just over 24 hours to complete and normally takes place in the part of the Fallopian Tube closest to the ovary. Fertilization occurs when sperm and egg fuse to form a new, genetically distinct male or female organism. In this first stage, the embryo, complete with two sets of DNA, is formally called a Zygote.


Day 2-3: The Zygote then enters into continuous cell division as it travels down the Fallopian Tube towards the uterus. When it reaches to about 12-32 cells, it is now formally called a Morula and measures only 0.1 to 0.2 mm. These individual cells (also known as Blastomeres) are in a compact ball, which are held together by a protective membrane called the zona pellucida (ie. like a balloon holding together a bunch of marbles).


Day 4: Fluid, then, begins to fill inside the ball of cells, creating a fluid-filled space called a blastocystic cavity. Because of the fluid, the dividing cells are pushed aside and form into two different groups: the first (outer) group will be responsible for implanting into the uterus and forming the placenta, while the second (inner) group of cells are responsible for forming your baby. The Embryo is now formally called a Blastocyst and has entered the inside of the Endometrium of the Uterus.


Day 5-6: The zona pellucida (the outer covering) then breaks open and the cells (now numbering over 100) move out, or "hatch" and get ready to implant into the uterus.

Day 7 (Implantation): The embryo implants into the endometrial lining of the uterus and burrows until it is protectively covered by the endometrium. This process continues into the second week of pregnancy.

Number 9 is the endometrial plug completely covering the implanted embryo and keeping it protected and Number 8 & 11 are the inner and outer layers of cells.
Week 2: Your baby now measures 0.2 mm in size. Blood vessels from the uterus begin to respond to the implanting embryo and fluid starts to accumulate (Number 8). The amniotic cavity (which holds your baby and contains amniotic fluid, Number 5) starts to form, along with other structures that provide nutrients to help your baby grow.

The cells that form your baby continue to divide and organize into two distinct layers. The outer layer of cells, called the epiblast (the blue cells in the picture) and the inner layer of cells called the hypoblast (the yellow cells in the picture). At the end of this week, a long streak appears in the middle of the epiblast layer (much like a long gap), called the primitive streak. The cells from the epiblast layer move into this streak to form a third, middle layer of cells (see the 4th picture below).


The primitive streak also designates what will be the head and the bottom, with migrating cells designating the left and the right sides of the body.

 Number 1 is the Primitive streak, Number 2 is the Epiblast layer, Number 3 is the space that is to be filled by the middle layer, Number 4 are the cells from the Epiblast layer replacing part of the Hypblast layer, Number 5 is the forming middle layer of cells and Number 6 is the Hypoblast layer.
Number 1 is the Primitive streak, Number 2 is the Epiblast layer, Number 3 is the space that is to be filled by the middle layer, Number 4 are the cells from the Epiblast layer replacing part of the Hypblast layer, Number 5 is the forming middle layer of cells and Number 6 is the Hypoblast layer.


Week 3: Your baby now measures 0.4 mm in size. The three layers of cells are now present and are given the following names: ectoblast (outer layer), mesoblast (middle layer), endoblast (inner layer). The hypoblast layer is partially replaced by the migrating cells from the epiblast, with the un-replaced hypoblast cells given the responsibility of forming the umbilical cord and the inside of the placenta sac. With the primitive streak visible, the left and right sides of the embryo and the top and bottom can be identified. By the end of the this week, the primitive streak begins to form the brain stem, with the surrounding Ectoderm layer beginning to form the different parts of the brain. The Mesoderm layer also begins forming the heart and gut.


Week 4: Your baby measures 5 mm. The primitive streak is completely closed, forming a tube that becomes the spinal cord. The head and brain continue to develop, along with the different parts of the gut (ie. all of the tubes going from your mouth to your anus). The 4 different areas of the heart and blood vessels can also be identified, with the heart beginning to beat. Other structures, such as the liver, umbilical, early upper limbs begin to develop, in addition to the skin, thyroid, diaphragm and the formation of the eyes.


Week 4: Your baby measures 5 mm. The primitive streak is completely closed, forming a tube that becomes the spinal cord. The head and brain continue to develop, along with the different parts of the gut (ie. all of the tubes going from your mouth to your anus). The 4 different areas of the heart and blood vessels can also be identified, with the heart beginning to beat. Other structures, such as the liver, umbilical, early upper limbs begin to develop, in addition to the skin, thyroid, diaphragm and the formation of the eyes.
Some women may also notice a missed period during this time and suspect pregnancy. Watch a live video of a baby at 4 weeks!




Week 5: Your baby measures up to 7 mm. We see many new structures forming, such as the lungs, inner ear, nose, genitals, abdomen, stomach, esophagus, trachea, brain structures (such as the hypothalamus and nerves), and arteries and veins. The legs and arms continue to elongate and develop, the eyes continue to form, and the physical appearance is becoming more recognizable.


Week 6: Your baby measure 11-14 mm. During this week, we see the formation of muscle, the tongue, eyelid grooves (where the eyelids will form), nerve specialization (ie. nerves for smell), ribs, the thymus and the start of the hands and feet.
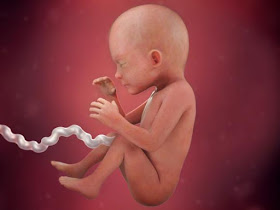
Most women find out they are pregnant at this point; when nausea begins. As you can see, her baby already has many physical body structures, including a well established nervous system and heart beat. Her baby is far from a "blob of cells!



Week 7: During this week, the leg bones and muscles develop and we can see movement of the limbs. The four chambered heart is now complete. We see other bone structures, such as the clavicle, vertebral discs, scapula (back of shoulder) form. We also see the kidneys and urinary bladder become established. The eyelids also form and cover the developing eye by the end of this week.

Week 8: This is the last week of the Embryonic Period. During this week, your baby's bones begin to harden. Their arms and legs are elingating, along with their fingers and toes. If it's a girl, her uterus and vagina start to fuse. If it's a boy, the testes begin producing testosterone and androstenedione. The intestines are pushed outside of the belly, where the umbilical cord attaches because the liver is so big that it takes up most of the room inside the abdomen. Nerves penetrate the tongue and nose, establishing taste and smell. Your baby's body is also becoming longer and straighter.



Week 6: Your baby measure 11-14 mm. During this week, we see the formation of muscle, the tongue, eyelid grooves (where the eyelids will form), nerve specialization (ie. nerves for smell), ribs, the thymus and the start of the hands and feet.
Most women find out they are pregnant at this point; when nausea begins. As you can see, her baby already has many physical body structures, including a well established nervous system and heart beat. Her baby is far from a "blob of cells!



Week 7: During this week, the leg bones and muscles develop and we can see movement of the limbs. The four chambered heart is now complete. We see other bone structures, such as the clavicle, vertebral discs, scapula (back of shoulder) form. We also see the kidneys and urinary bladder become established. The eyelids also form and cover the developing eye by the end of this week.

Week 8: This is the last week of the Embryonic Period. During this week, your baby's bones begin to harden. Their arms and legs are elingating, along with their fingers and toes. If it's a girl, her uterus and vagina start to fuse. If it's a boy, the testes begin producing testosterone and androstenedione. The intestines are pushed outside of the belly, where the umbilical cord attaches because the liver is so big that it takes up most of the room inside the abdomen. Nerves penetrate the tongue and nose, establishing taste and smell. Your baby's body is also becoming longer and straighter.

Watch more videos here!


Week 9 (Start of the Fetal Stage!): Your baby is now called a Fetus. As mentioned before, during the first 8 weeks of your pregnancy, over 90% of the 4500 designated structures of the adult body are already established. During the fetal period the organs that formed during the embryonic period grow and differentiate, in a process called: organogenesis. Most women who suspect they are pregnant will have their first ultrasound and pregnancy test at the doctor's office. During the ultrasound, they will be able to see the pitter-patter of the baby's fast heart beat.
During this week, your baby's toes and fingers become separate as the webbing between them disappears. The eyelids continue to cover and fuse over your baby's developing eyes and the major parts of their brain are well-established. All major structures and organs continue to grow and mature.

Week 10: Your baby's intestines are now back inside their body. Finger nails begin to grow, the outside of the ear and distinct facial features can be seen, the legs become longer, and the growth hormone (produced by the pituitary gland in the brain) is detectable. The pancreas also begins to produce insulin.


Week 11: Your baby can now make different, complex facial expressions. Their nose and lips are also fully formed and their genitalia are fully formed. However, sometimes the clitoris on girls can be confused with the penis on boys on ultrasound. By 17 weeks, gender confirmation is more accurate.

Week 12: Your baby's weight has increased by 60% and measures 12 cm from the top of their head to the heel of their foot. Movement has also increased, with your baby touching their face up to 50 times and hour. The immune system is also maturing as the T-cells leave the Thymus and move throughout the body. Taste buds are established, the arms and legs have reached their proper proportions, the bowel begins to function, the hard and soft palate of the mouth are completely fused, and the lungs begin to secrete surfactant (an important substance that keeps our lungs from collapsing during breathing).


Week 13: This week begin the Second Trimester! Your baby now measures 15 cm from the top of their head to the heel of their foot. Their teeth continue to form, hearing continues to mature, and touch has become very sensitive.


Week 14: Your baby now measures 17 cm from the top of the their head to the heel of their foot. Their cheeks start to fatten up during this week and their brain starts to show four distinct lobes. Toe nails also appear, mouth movements can bee seen (with girls moving their jaws more often than boys), kidneys are fully functioning and your baby responds to light touch. If you are having a girl, her ovaries already contain 2 million eggs.

Week 15: Your baby now measures 19.5 cm from the top of the their head to the heel of their foot. Fat starts to deposit throughout the rest of the body (as glucagon is produced by the pancreas) and stem cells are seen within the bone marrow (where blood cells and most immune cells are made). Your baby's eyes are still closed, but they may be seen reacting to light coming through your belly.

Week 16: Your baby now measures 21 cm from the top of the their head to the heel of their foot. During this week, you may be able to feel your baby move. Enamel (what makes our teeth hard) starts to develop over the developing teeth and the airways within the lungs (bronchial tree) are now fully formed. The different layers of the skin also begin to form, along with hair follicles and the hardening nails. Any pain experienced by your baby will now trigger the release of stress hormones by the child's body.


Week 17: The eyes are now well advanced, with the retina displaying distinct layers. Your baby's skeleton is fully hardened and their joints are more easily movable.

Week 18: A protective white substance, called vernix caseosa covers your baby, protecting their skin from exposure to amniotic fluid. Sweat glands are also forming, insulin is fully produced by the pancreas and the the two sides of the brain are now connected by a band of neural fibers called the corpus callosum. Your baby's vocal cords can also be seen moving as if they were talking or crying. The ears are now nearly complete and in their correct position.


Week 19: If you are having a girl, the number of eggs contained within her ovaries has reached its peak number of 7 million eggs. By the time she is born, this number will have decreased to about 2 million. Your baby's movements, breathing activity, and heart rate also begin to follow daily cycle. REM sleep may also be observed around this time.

Week 20: Your baby now measures 28 cm from the top of the their head to the heel of their foot and they can now hear the sound of your voice! Hair can also be seen covering your baby's body and the swallowing of amniotic fluid starts the production of meconium (baby's first poop) within their bowel.


Week 21: Your baby's movements are very noticeable by this point. The outer layer of their skin, called the stratum corneum, consists of dead skin cells that may fall off and float within the amniotic fluid. Baby's born during this week may have a small chance of survival.

Week 22: Your baby's spleen is now more organized and infiltrated with the T and B immune cells. Breathing motions may also begin during this week, as amniotic fluid is drawn into their lungs. The amount of "breaths" taken per minute depends on the mother's CO2 and Oxygen levels within her own blood stream. This is why smoking can have detrimental effects on your baby's growth, since it decreases the amount of oxygen available to the baby.

Week 23: More energy is starting to be put towards the growth of your baby's brain, which weighs 100 grams by this point. Their hearing is much more in tune with specific sounds and voices. When they are born, they may react to familiar sounds they remember hearing while in the womb.
Week 24: Your baby now measures 34.5 cm from the top of the their head to the heel of their foot and has a higher chance of survival if they are born during this week. Surfactant is being secreted by the lung cells, which makes it possible for gas exchange to occur during breathing. The eyelids also re-open and your baby may begin to start blinking. Your baby may also become startled with loud noises and react to other stimuli, such as pressure, movement, pain, hot/cold temperatures, taste and light. Their brain also takes off on a growth spurt, consuming more than 50 percent of the energy used by your baby, resulting in a brain weight increase between 400% and 500%. Some permanent teeth may also be seen underneath the gums, namely the incisors and canines.

Week 25: Your baby's eyes now have over 100 million rods and 7 million cones in each eye that help detect light levels and colors. Your baby can also taste what your eat. For instance, amniotic fluid assumes the odor of garlic within 45 minutes of ingestion by pregnant women, which your baby may react to.

Week 26: Your baby is looking less wrinkled and more plump as they gain body fat. Tears can now be produced from the tear ducts next to the eyes and your baby's sense of smell is now established.

Week 27: Your baby's pupils can now dilate and constrict in response to light and their eyelids may already sport some eyelashes. Their brain is also very active as your baby experiences a regular wake-sleep cycle.


Week 28: This week begins the Third Trimester and your baby now measures 39.5 cm from the top of the their head to the heel of their foot. The air sacs within their lungs are multiplying and their ears can now distinguish different pitches of sound.
The third trimester is primarily a growth and fattening stage. The brown fat that is deposited is quickly used by your baby's body to supply the large amount of energy needed after birth. This fat is, then, replaced by the yellow fat that is stored within everyone's body.


Week 29: Your baby's pre-molars appear during this week. Their frequent movements allow their muscles to become stronger, their lungs continue to mature and their head continues to enlarge to accommodate their rapidly growing brain.

Week 30: Breathing movements become more common during this week, occurring 30 – 40 percent of the time. If your are having a boy, then his testes (which are currently in the abdomen) begin to descend into the scrotum. Your baby's growing head also measures 30 cm in circumference.

Week 31: Your baby is now able to freely move their head from side-to-side. Fat continues to be deposited throughout their body, with your baby even developing a food preference based on what mommy eats.

Week 32: Your baby now measures 45 cm from the top of the their head to the heel of their foot and they can now store memories and form preferences for certain sounds, such a music and voices. The blood-filtering network within their kidneys (called Glomeruli) are established and their finger nails have reached the tip of their fingers.

Week 33: Folds within your baby's brain continue to form, increasing the surface area to volume ratio of their brain within the skull. Your baby also begins to rapidly put on weight, in preparation for the outside world.

Week 34: If your baby is born during this week, and has no other health problems, they usually do very well. The nervous system continues to mature and the nerves begin to be coated with a layer of phospholipids, cholesterol and proteins called the myelin sheath. This enhances the amount of communication between neurons and serves as a protective layer.

Week 35: The amount of amniotic fluid has reached its peak. As your baby nears the 40 week mark, the amount of fluid does decrease as your baby continues to take up more space. Their kidneys are also fully mature at this point and their liver can process some waste products. They also have a very strong "kung-fu" grip and may be seen grabbing onto their umbilical cord or other body parts.

Week 36: Your baby now measures 48.5 cm from the top of the their head to the heel of their foot. Their brain weighs 300 grams and their body should be gaining about 1 ounce per day. The lungs are producing surfactant at an accelerated rate and the vernix casosa that covered their skin (to protect it from the amniotic fluid) starts to shed off.


Week 37: Your baby is drinking about 15 oz (or 450cc) of amniotic fluid each day. The lungs and brain are in the final stages of maturation as your baby prepares for survival outside the womb.


Clinician previously considered the 37 week mark as full term. However, further understanding of the developmental process during these later weeks has led to a further breakdown in terminology between the 37th and 42nd week, which is as follows:
Early Term: Between 37 weeks 0 days and 38 weeks 6 days
Full Term: Between 39 weeks 0 days and 40 weeks 6 days
Late Term: Between 41 weeks 0 days and 41 weeks 6 days
Post-term: Between 42 weeks 0 days and beyond
Week 38-40: Your baby now measures 50 cm from the top of the their head to the heel of their foot and their head circumference is about 35 cm. Their umbilical cord typically measures between 20 to 24 inches (50 to 60 cm) and their brain now weighs 350 grams. When labor is initiated, your baby transitions from a fetus to a newborn. Powerful contractions of the uterus result in childbirth and the expulsion of the placenta, which now weighs about 1/6th as much as the newborn. At birth, the oxygen received through the placenta is, then, replaced by air coming through the lungs.



Between fertilization and birth, your baby's heart beats approximately 54 million times. During the course of an 80-year lifespan, your heart only beats over 3.2 billion times. Below is a picture displaying the rapid growth of the human brain during gestation:

This youtube video also contains a compilation of real-time photographs of human gestation:
Short Answer: There is absolutely no magical portal to go through to turn someone into a human being. Our entire existence begins when sperm meets egg, starting the process of "Human Development;" creating a distinct and unique human being. Destroying that human being during ANY part of their existence destroys that unique individual forever; meaning they are Never coming back! By the time most women realize they are pregnant (between week 4-6) the cellular stage has been far surpassed. By week 4 we have a functioning heart beat and by week 6 we start to see hands and feet. The lack of knowledge and understanding of human development is what fuels the pro-choice/pro-abortion agenda. These children must be recognized as distinct human beings, worthy of value and protection from those who wish to harm them.
References and pictures:
http://www.embryology.ch/indexen.html
https://embryology.med.unsw.edu.au/embryology/index.php/Timeline_human_development
http://www.ehd.org/virtual-human-embryo/
https://www.ehd.org/science_main.php
https://www.babycenter.com/fetal-development-week-by-week
https://www.innerbaia.com/Embryo/hum_emb.htm
http://www.webmd.com/baby/ss/slideshow-fetal-development
6. OTHER COMMON PRO-CHOICE/PRO-ABORTION ARGUMENTS
Below are some other run-of-the-mill pro-abortion arguments that you may see; which can be quickly answered in just a few sentences.
Myth: Defunding Planned Parenthood would hurt women and their access to affordable healthcare!
Truth: The tax dollars pulled away from abortion giants, like Planned Parenthood, would actually be put towards Federally Qualified Health Centers that would provide even more free/affordable services to women and their families, without promoting abortion. Therefore, this shift would be better for women and their healthcare needs! Find your nearest FQHC here.
Myth: Abortion is okay if the baby is "unwanted"
Truth: Just as with a child conceived in rape/incest, there are no physical differences between a wanted and an unwanted baby. In fact, no baby is ever truly unwanted. There are hundreds of families waiting to adopt, with most couples frequently requesting infants. Not being emotionally wanted by the biological parent is no reason to kill a child.
Myth: There are so many unwanted children in Foster Care already!
Truth: As stated in one of my previous blog posts, the purpose behind the foster care system is to eventually reunite biological children with their biological families. In fact, 50% of children in the foster care system are eventually reunited with their parent(s) or a biological family member, with 25% adopted by the foster parents themselves, leaving only 25% of children waiting for adoption. Adopting through the foster system is, also, basically free to the adopting family, or at least covered by the state. We only hear about the "bad" foster homes in the news because the hundreds of fantastic foster families are not news worthy. Again, this is not an adequate excuse to end a child's life.
Myth: You can't be a Pro-Life and a Feminist!
Truth: True Feminism Is Pro-life! In fact, our founding mothers of the feminist movement were even Pro-life. But, today's modern day feminism has taken on a more "male-like" complex; completely excluding our pregnant mothers and forming this supremacy over the one organ that makes us biologically female: the uterus. Some women shout "I am more than my uterus!" I say, "well, that's great, but don't disrespect the uterus either!" The female body is capable of bringing life into this world; that should be something to be proud of! Now, I'm not saying every female needs to go out and get pregnant, but we don't need a culture that shames or abandons them either. We need to defend and fight for our mothers, protect our children and future mothers and support those who want to have a family and a sustainable career. I, for one, had my eldest while in college and was still able to pursue my career with very little assistance. It was hard, but not impossible, and I do wish some things (like discounted childcare, extra loan funding, easier and quicker access to the WIC program etc.) were more accessible. Women should not feel forced to choose between a career and a family. We need a country that is more family oriented so that women can easily have both!
Children don't ruin lives, they give you a new ones!-Wanda Sykes. Children may even be the driving force you need to accomplish your goals in life; as my children were.
Myth: Abortion is okay if the mother's life is in danger.
Truth: These types of cases are actually very rare and no case is the same as the next. In the majority of these cases, both the mother's and the child's life can be saved. The goal, here, is to sustain the mother's pregnancy for as long as possible until her baby has the highest chance of surviving outside of the womb. At that point, the mother will be induced early and then treated.
There's always a better way to solving a problem. Abortion only seems to be the easiest and quickest "solution" that doctors have a tendency to jump to. It's not their child, so why would they care?
Myth: The baby isn't even viable until 24 weeks, so abortion is okay until then!
Truth: First of all, that child is completely "viable" inside the womb. You can not blame or punish this child for not being able to survive in an environment it is not ready for! Would you expect a child at any other age to accomplish the same tasks as an adult?! That is developmental discrimination! Dependency, also, does not equal property. These children are not possessions that you own and dispose of as you wish, all because they are dependent on someone for shelter, protection and nourishment. If that were the case, then we would have a different perspective on coma and elderly patients. Viability does not dictate Personhood!
Myth: Abortion is okay if they child has a disability or genetic defect.
Truth: I say this with emphasis: Abortion is Not a Merciful Act! As we saw in my description of human development, above, one of the very first structures to form is the nervous system. As these nerves grow and mature, their sensitivities to certain stimuli change. In other words, an unborn child's nerve receptors are more sensitive than that of a young child's or adult's. A light touch to a fetus, for example, may feel more extreme than a light touch to someone outside the womb. Now, imagine the very first time an unborn child experiences pain through abortion. Not only is this their first time ever feeling pain, but this pain is felt at a more intense and higher level. It's not merciful to make your child experience something like that, even if they are going to die anyways, once they are born. The most humane thing you could do is to allow them to live, however long that may be, with love felt all around them. Baby hospices even exist for situations like these. Any pain that this child would experience outside the womb, is nothing compared to the pain they would feel during an abortion.
Please list any questions or comments below, or, visit my facebook page, link listed on the right menu bar. Thank you for being defenders of LIFE! -VLM
During this week, your baby's toes and fingers become separate as the webbing between them disappears. The eyelids continue to cover and fuse over your baby's developing eyes and the major parts of their brain are well-established. All major structures and organs continue to grow and mature.

Week 10: Your baby's intestines are now back inside their body. Finger nails begin to grow, the outside of the ear and distinct facial features can be seen, the legs become longer, and the growth hormone (produced by the pituitary gland in the brain) is detectable. The pancreas also begins to produce insulin.


Week 11: Your baby can now make different, complex facial expressions. Their nose and lips are also fully formed and their genitalia are fully formed. However, sometimes the clitoris on girls can be confused with the penis on boys on ultrasound. By 17 weeks, gender confirmation is more accurate.

Week 12: Your baby's weight has increased by 60% and measures 12 cm from the top of their head to the heel of their foot. Movement has also increased, with your baby touching their face up to 50 times and hour. The immune system is also maturing as the T-cells leave the Thymus and move throughout the body. Taste buds are established, the arms and legs have reached their proper proportions, the bowel begins to function, the hard and soft palate of the mouth are completely fused, and the lungs begin to secrete surfactant (an important substance that keeps our lungs from collapsing during breathing).


Week 13: This week begin the Second Trimester! Your baby now measures 15 cm from the top of their head to the heel of their foot. Their teeth continue to form, hearing continues to mature, and touch has become very sensitive.


Week 14: Your baby now measures 17 cm from the top of the their head to the heel of their foot. Their cheeks start to fatten up during this week and their brain starts to show four distinct lobes. Toe nails also appear, mouth movements can bee seen (with girls moving their jaws more often than boys), kidneys are fully functioning and your baby responds to light touch. If you are having a girl, her ovaries already contain 2 million eggs.

Week 15: Your baby now measures 19.5 cm from the top of the their head to the heel of their foot. Fat starts to deposit throughout the rest of the body (as glucagon is produced by the pancreas) and stem cells are seen within the bone marrow (where blood cells and most immune cells are made). Your baby's eyes are still closed, but they may be seen reacting to light coming through your belly.

Week 16: Your baby now measures 21 cm from the top of the their head to the heel of their foot. During this week, you may be able to feel your baby move. Enamel (what makes our teeth hard) starts to develop over the developing teeth and the airways within the lungs (bronchial tree) are now fully formed. The different layers of the skin also begin to form, along with hair follicles and the hardening nails. Any pain experienced by your baby will now trigger the release of stress hormones by the child's body.


Week 17: The eyes are now well advanced, with the retina displaying distinct layers. Your baby's skeleton is fully hardened and their joints are more easily movable.

Week 18: A protective white substance, called vernix caseosa covers your baby, protecting their skin from exposure to amniotic fluid. Sweat glands are also forming, insulin is fully produced by the pancreas and the the two sides of the brain are now connected by a band of neural fibers called the corpus callosum. Your baby's vocal cords can also be seen moving as if they were talking or crying. The ears are now nearly complete and in their correct position.


Week 19: If you are having a girl, the number of eggs contained within her ovaries has reached its peak number of 7 million eggs. By the time she is born, this number will have decreased to about 2 million. Your baby's movements, breathing activity, and heart rate also begin to follow daily cycle. REM sleep may also be observed around this time.

Week 20: Your baby now measures 28 cm from the top of the their head to the heel of their foot and they can now hear the sound of your voice! Hair can also be seen covering your baby's body and the swallowing of amniotic fluid starts the production of meconium (baby's first poop) within their bowel.


Week 21: Your baby's movements are very noticeable by this point. The outer layer of their skin, called the stratum corneum, consists of dead skin cells that may fall off and float within the amniotic fluid. Baby's born during this week may have a small chance of survival.

Week 22: Your baby's spleen is now more organized and infiltrated with the T and B immune cells. Breathing motions may also begin during this week, as amniotic fluid is drawn into their lungs. The amount of "breaths" taken per minute depends on the mother's CO2 and Oxygen levels within her own blood stream. This is why smoking can have detrimental effects on your baby's growth, since it decreases the amount of oxygen available to the baby.

Week 23: More energy is starting to be put towards the growth of your baby's brain, which weighs 100 grams by this point. Their hearing is much more in tune with specific sounds and voices. When they are born, they may react to familiar sounds they remember hearing while in the womb.

Week 24: Your baby now measures 34.5 cm from the top of the their head to the heel of their foot and has a higher chance of survival if they are born during this week. Surfactant is being secreted by the lung cells, which makes it possible for gas exchange to occur during breathing. The eyelids also re-open and your baby may begin to start blinking. Your baby may also become startled with loud noises and react to other stimuli, such as pressure, movement, pain, hot/cold temperatures, taste and light. Their brain also takes off on a growth spurt, consuming more than 50 percent of the energy used by your baby, resulting in a brain weight increase between 400% and 500%. Some permanent teeth may also be seen underneath the gums, namely the incisors and canines.

Week 25: Your baby's eyes now have over 100 million rods and 7 million cones in each eye that help detect light levels and colors. Your baby can also taste what your eat. For instance, amniotic fluid assumes the odor of garlic within 45 minutes of ingestion by pregnant women, which your baby may react to.

Week 26: Your baby is looking less wrinkled and more plump as they gain body fat. Tears can now be produced from the tear ducts next to the eyes and your baby's sense of smell is now established.

Week 27: Your baby's pupils can now dilate and constrict in response to light and their eyelids may already sport some eyelashes. Their brain is also very active as your baby experiences a regular wake-sleep cycle.


Week 28: This week begins the Third Trimester and your baby now measures 39.5 cm from the top of the their head to the heel of their foot. The air sacs within their lungs are multiplying and their ears can now distinguish different pitches of sound.
The third trimester is primarily a growth and fattening stage. The brown fat that is deposited is quickly used by your baby's body to supply the large amount of energy needed after birth. This fat is, then, replaced by the yellow fat that is stored within everyone's body.


Week 29: Your baby's pre-molars appear during this week. Their frequent movements allow their muscles to become stronger, their lungs continue to mature and their head continues to enlarge to accommodate their rapidly growing brain.

Week 30: Breathing movements become more common during this week, occurring 30 – 40 percent of the time. If your are having a boy, then his testes (which are currently in the abdomen) begin to descend into the scrotum. Your baby's growing head also measures 30 cm in circumference.

Week 31: Your baby is now able to freely move their head from side-to-side. Fat continues to be deposited throughout their body, with your baby even developing a food preference based on what mommy eats.

Week 32: Your baby now measures 45 cm from the top of the their head to the heel of their foot and they can now store memories and form preferences for certain sounds, such a music and voices. The blood-filtering network within their kidneys (called Glomeruli) are established and their finger nails have reached the tip of their fingers.

Week 33: Folds within your baby's brain continue to form, increasing the surface area to volume ratio of their brain within the skull. Your baby also begins to rapidly put on weight, in preparation for the outside world.

Week 34: If your baby is born during this week, and has no other health problems, they usually do very well. The nervous system continues to mature and the nerves begin to be coated with a layer of phospholipids, cholesterol and proteins called the myelin sheath. This enhances the amount of communication between neurons and serves as a protective layer.

Week 35: The amount of amniotic fluid has reached its peak. As your baby nears the 40 week mark, the amount of fluid does decrease as your baby continues to take up more space. Their kidneys are also fully mature at this point and their liver can process some waste products. They also have a very strong "kung-fu" grip and may be seen grabbing onto their umbilical cord or other body parts.

Week 36: Your baby now measures 48.5 cm from the top of the their head to the heel of their foot. Their brain weighs 300 grams and their body should be gaining about 1 ounce per day. The lungs are producing surfactant at an accelerated rate and the vernix casosa that covered their skin (to protect it from the amniotic fluid) starts to shed off.


Week 37: Your baby is drinking about 15 oz (or 450cc) of amniotic fluid each day. The lungs and brain are in the final stages of maturation as your baby prepares for survival outside the womb.


Clinician previously considered the 37 week mark as full term. However, further understanding of the developmental process during these later weeks has led to a further breakdown in terminology between the 37th and 42nd week, which is as follows:
Early Term: Between 37 weeks 0 days and 38 weeks 6 days
Full Term: Between 39 weeks 0 days and 40 weeks 6 days
Late Term: Between 41 weeks 0 days and 41 weeks 6 days
Post-term: Between 42 weeks 0 days and beyond
Week 38-40: Your baby now measures 50 cm from the top of the their head to the heel of their foot and their head circumference is about 35 cm. Their umbilical cord typically measures between 20 to 24 inches (50 to 60 cm) and their brain now weighs 350 grams. When labor is initiated, your baby transitions from a fetus to a newborn. Powerful contractions of the uterus result in childbirth and the expulsion of the placenta, which now weighs about 1/6th as much as the newborn. At birth, the oxygen received through the placenta is, then, replaced by air coming through the lungs.



Between fertilization and birth, your baby's heart beats approximately 54 million times. During the course of an 80-year lifespan, your heart only beats over 3.2 billion times. Below is a picture displaying the rapid growth of the human brain during gestation:

This youtube video also contains a compilation of real-time photographs of human gestation:
Short Answer: There is absolutely no magical portal to go through to turn someone into a human being. Our entire existence begins when sperm meets egg, starting the process of "Human Development;" creating a distinct and unique human being. Destroying that human being during ANY part of their existence destroys that unique individual forever; meaning they are Never coming back! By the time most women realize they are pregnant (between week 4-6) the cellular stage has been far surpassed. By week 4 we have a functioning heart beat and by week 6 we start to see hands and feet. The lack of knowledge and understanding of human development is what fuels the pro-choice/pro-abortion agenda. These children must be recognized as distinct human beings, worthy of value and protection from those who wish to harm them.
References and pictures:
http://www.embryology.ch/indexen.html
https://embryology.med.unsw.edu.au/embryology/index.php/Timeline_human_development
http://www.ehd.org/virtual-human-embryo/
https://www.ehd.org/science_main.php
https://www.babycenter.com/fetal-development-week-by-week
https://www.innerbaia.com/Embryo/hum_emb.htm
http://www.webmd.com/baby/ss/slideshow-fetal-development
6. OTHER COMMON PRO-CHOICE/PRO-ABORTION ARGUMENTS
Below are some other run-of-the-mill pro-abortion arguments that you may see; which can be quickly answered in just a few sentences.
Myth: Defunding Planned Parenthood would hurt women and their access to affordable healthcare!
Truth: The tax dollars pulled away from abortion giants, like Planned Parenthood, would actually be put towards Federally Qualified Health Centers that would provide even more free/affordable services to women and their families, without promoting abortion. Therefore, this shift would be better for women and their healthcare needs! Find your nearest FQHC here.
Myth: Abortion is okay if the baby is "unwanted"
Truth: Just as with a child conceived in rape/incest, there are no physical differences between a wanted and an unwanted baby. In fact, no baby is ever truly unwanted. There are hundreds of families waiting to adopt, with most couples frequently requesting infants. Not being emotionally wanted by the biological parent is no reason to kill a child.
Myth: There are so many unwanted children in Foster Care already!
Truth: As stated in one of my previous blog posts, the purpose behind the foster care system is to eventually reunite biological children with their biological families. In fact, 50% of children in the foster care system are eventually reunited with their parent(s) or a biological family member, with 25% adopted by the foster parents themselves, leaving only 25% of children waiting for adoption. Adopting through the foster system is, also, basically free to the adopting family, or at least covered by the state. We only hear about the "bad" foster homes in the news because the hundreds of fantastic foster families are not news worthy. Again, this is not an adequate excuse to end a child's life.
Myth: You can't be a Pro-Life and a Feminist!
Truth: True Feminism Is Pro-life! In fact, our founding mothers of the feminist movement were even Pro-life. But, today's modern day feminism has taken on a more "male-like" complex; completely excluding our pregnant mothers and forming this supremacy over the one organ that makes us biologically female: the uterus. Some women shout "I am more than my uterus!" I say, "well, that's great, but don't disrespect the uterus either!" The female body is capable of bringing life into this world; that should be something to be proud of! Now, I'm not saying every female needs to go out and get pregnant, but we don't need a culture that shames or abandons them either. We need to defend and fight for our mothers, protect our children and future mothers and support those who want to have a family and a sustainable career. I, for one, had my eldest while in college and was still able to pursue my career with very little assistance. It was hard, but not impossible, and I do wish some things (like discounted childcare, extra loan funding, easier and quicker access to the WIC program etc.) were more accessible. Women should not feel forced to choose between a career and a family. We need a country that is more family oriented so that women can easily have both!
Children don't ruin lives, they give you a new ones!-Wanda Sykes. Children may even be the driving force you need to accomplish your goals in life; as my children were.
Myth: Abortion is okay if the mother's life is in danger.
Truth: These types of cases are actually very rare and no case is the same as the next. In the majority of these cases, both the mother's and the child's life can be saved. The goal, here, is to sustain the mother's pregnancy for as long as possible until her baby has the highest chance of surviving outside of the womb. At that point, the mother will be induced early and then treated.
There's always a better way to solving a problem. Abortion only seems to be the easiest and quickest "solution" that doctors have a tendency to jump to. It's not their child, so why would they care?
Myth: The baby isn't even viable until 24 weeks, so abortion is okay until then!
Truth: First of all, that child is completely "viable" inside the womb. You can not blame or punish this child for not being able to survive in an environment it is not ready for! Would you expect a child at any other age to accomplish the same tasks as an adult?! That is developmental discrimination! Dependency, also, does not equal property. These children are not possessions that you own and dispose of as you wish, all because they are dependent on someone for shelter, protection and nourishment. If that were the case, then we would have a different perspective on coma and elderly patients. Viability does not dictate Personhood!
Myth: Abortion is okay if they child has a disability or genetic defect.
Truth: I say this with emphasis: Abortion is Not a Merciful Act! As we saw in my description of human development, above, one of the very first structures to form is the nervous system. As these nerves grow and mature, their sensitivities to certain stimuli change. In other words, an unborn child's nerve receptors are more sensitive than that of a young child's or adult's. A light touch to a fetus, for example, may feel more extreme than a light touch to someone outside the womb. Now, imagine the very first time an unborn child experiences pain through abortion. Not only is this their first time ever feeling pain, but this pain is felt at a more intense and higher level. It's not merciful to make your child experience something like that, even if they are going to die anyways, once they are born. The most humane thing you could do is to allow them to live, however long that may be, with love felt all around them. Baby hospices even exist for situations like these. Any pain that this child would experience outside the womb, is nothing compared to the pain they would feel during an abortion.
Please list any questions or comments below, or, visit my facebook page, link listed on the right menu bar. Thank you for being defenders of LIFE! -VLM
No comments:
Post a Comment